Elizabeth B Gilbert, MD
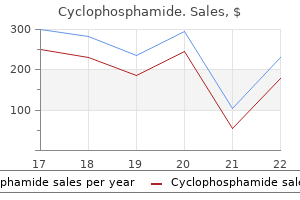
 https://medicine.duke.edu/faculty/elizabeth-b-gilbert-md Figure 1 Diagnostic workup in patients presenting with sustained ventricular tachycardia or ventricular brillation symptoms 0f parkinson disease cyclophosphamide 50 mg on-line. Occasional studies mediated triggering mechanisms treatment mastitis order 50mg cyclophosphamide with mastercard, slowing of the sinus rate and pos with amiodarone have shown positive results treatment in statistics cheap cyclophosphamide 50mg on-line, but this is not a con sibly inhibition of excess calcium release by the ryanodine receptor sistent nding treatment uterine fibroids order cyclophosphamide 50mg fast delivery. However, reduction of ar longer the therapy and the higher the dose of amiodarone, the rhythmic death does not seem to be associated with a reduction greater the likelihood that adverse side effects will require discon in total mortality, and adverse events associated with amiodarone tinuation of the drug. Several drugs, such as angiotensin satisfactory suppression of arrhythmia episodes. A meta-analysis of the three trials demonstrated 149 ing inappropriate shocks, which are especially frequent in children. The electrode is positioned so that the Wearable cardioverter debrillator distal part of the lead is placed at the left parasternal edge and the device is placed over the fth intercostal space between Recommendation Classa Levelb Ref. The precise electrode con guration used for sensing can be congured by programming. In one of the largest trials, 330 patients, 304 of implant, peripartum cardiomyopathy, active myocarditis and arrhythmias in whom were successfully implanted, underwent appropriate deb the early post-myocardial infarction rillation testing and were successfully followed for a mean of 11 phase). Thirteen per cent of patients received an inappropriate shock due largely to supraventricular tachycardia or to T-wave An external debrillator (plus leads and electrode pads) attached to a oversensing, which has also been described in younger patient 160 wearable vest has been shown to successfully identify and interrupt groups. More recently, Ep ous pacing can be delivered by the device for 30 seconds after 170 stein et al. For example, individual studies have Public access debrillation presented a higher than average rate of inappropriate shocks 160 and complications requiring reintervention: whether these Recommendations Classa Levelb Ref. Prompt de brillation is much more likely than deferred debrillation to re store an organized rhythm and stable cardiac output. Overall, survival is better lished, especially in locations where crowds and stress are for patients presenting with ventricular tachyarrhythmias com common, and particularly where trained volunteers can be readily pared with asystole. Out-of hospital cardiac arrests occur most commonly (70%) in the sensus conference held in Dallas, Texas, in 2010. In the case home, even in younger patients,176 but these are infrequently wit of cardiac arrest, the universal algorithm should be applied nessed and therefore cannot be prevented by home-based (Figure 2). Implementation of automatic external debrillator programmes should be performed is still debatable. In cases of out-of-hospital reduces mortality in public places where cardiac arrests are usually cardiac arrest, cardiopulmonary resuscitation with chest compres 178 sion should be performed immediately until debrillation is witnessed. Basic and advanced life support activities have led to the generation of protocols to guide responders. In cases of in-hospital cardiac arrest, immediate debrilla published by the European Resuscitation Council and the Inter tion should be attempted because, in this case, the likelihood that national Consensus on Cardiopulmonary Resuscitation and Emer cardiac arrest is due to sustained ventricular tachyarrhythmia is gency Cardiovascular Care,179 cover the broad expanse of clinical greater. They provide Semi-automated debrillators provide an excellent technology to clear management information, and the reader is referred to the spread debrillation capability within hospitals. In patients Cardioversion or debrillation and acute treatment of who are hypotensive and yet conscious, immediate sedation should sustained ventricular arrhythmias be given before undergoing cardioversion. In patients with wide complex tachycardia who are haemodynamically stable, electrical Recommendations Classa Levelb Ref. Controlled debrillator trials demonstrated preserved or improved aClass of recommendation. Sup enced centres with preoperative and intraoperative electrophysio port from healthcare professionals mitigates these concerns, but logical mapping. Management of ventricular It is recommended that post-resuscitation care is performed arrhythmias and prevention of in high-volume expert centres capable sudden cardiac death in coronary of offering multidisciplinary intensive 245, care treatment, including primary I B artery disease 246 coronary interventions, electrophysiology, cardiac assist 5. In addition to quick death during the rst few hours after the onset of symptoms is and complete coronary revascularization, non-pharmacological in currently a major cause of mortality in acute myocardial terventions (cardioversion, debrillation, pacing and catheter abla infarction. Prevention and management of sudden cardiac death associated with acute coronary syndromes: in hospital phase. In patients with chest pain, it is A coronary angiogram followed, if recommended to reduce delays both necessary, by coronary angioplasty from symptom onset to rst medical I A 244 within 2 h of hospital admission is I C 13,250 contact and from rst medical contact to recommended in patients with high-risk reperfusion. Prevention and management of sudden cardiac death Prevention and management of sudden cardiac death associated with acute coronary syndromes: in-hospital associated with acute coronary syndromes: in-hospital phase. Pacing/implantable cardioverter debrillator ablation Recommendations Classa Levelb Ref. This section focuses on the specic role of reper lar ectopy can be a sign that further revascularization. Precise catheter mapping and successful ablation of triggers magnesaemia and hypokalaemia may help in selected patients. Assessment of up to ve-fold increase in hospital mortality and probably identi es a risk for longer-term mortality. They provide clear management information and the read er is referred to the source documents for details. Percutaneous coronary intervention is also associated with a marked decline in cardiac mortality driven by Recommendations Classa Levelb Ref. The effect on all-cause given its high incidence of drug toxicity,8 it is not recommended for mortality did not vary according to ischaemic or non-ischaemic general use in these patients. A relatively high proportion of these pa with non-ischaemic aetiologies a reduction in all-cause mortality and tients have non-cardiovascular co-morbidities, and although sudden arrhythmic mortality is supported as well. In the same trial also for patients with ischaemic aetiology, there was only a trend in the re 6. These 331 pharmacological therapy who are patients often have to wait at least 1 year and their risk of sudden expected to survive at least 1 year with death is high. Data from two observational studies that together ex good functional status, provided that 320 biventricular pacing as close as possible amined almost 2000 patients, one of them recent and the other 321 to 100% can be achieved. Cardiac resynchronization therapy and premature ventricular complex a debrillator in the primary prevention of sudden death in patients in sinus rhythm with mild (New York Recommendations Classa Levelb Ref. In addition, there is no consensus with discontinuation was more frequent in patients taking sotalol ora com respect to the ideal procedural endpoint. Cath eter ablation of one of the bundle branches is curative, although the right bundle branch is the preferred target, as it is more easily Risk stratication and management of patients with accessible for ablation. The incremental value of late treatment with optimal pharmacological 317, therapy who are expected to survive gadolinium enhancement over other prognostic markers needs to 354 for. Prevention of sudden cardiac death in patients with hypertrophic cardiomyopathy 7. The histological therapy, including long-term 395 hallmark of the disease is replacement of cardiomyocytes by adipose 382,383 complications, and the benet for the and brous tissue. The annual mortality rate reported in different c Reference(s) supporting recommendations. The two main types of cardiac amyloidosis are light-chain amyloid osis, caused by deposition of monoclonal light chains, and hereditary transthyretin-associated amyloidosis, in which normal (wild-type) 7. Elevated levels of cardiac troponins and N-terminal pro-B-type meta-analysis (18 studies) of 610 patients followed for a mean per natriuretic peptide are sensitive markers of cardiac involvement and pre iod of 3. Restrictive cardiomyopathy is the least common of all the cardiomyopathies 412 Recommendations Classa Levelb Ref. There are fewer data in adults, but reported survival rates are similar at 5 years. There are no prospective data on prophylactic implantation dysfunction and more advanced conduction abnormalities. In some patients, non-compaction is associated with ventricular dilatation and systolic dysfunction. In addition to a history of current illness medications hard on liver buy discount cyclophosphamide 50mg line, the history Whenever possible medicine evolution order cyclophosphamide 50 mg, direct and ongoing contact should be made should include (1) a review of available records symptoms 4 weeks pregnant generic 50mg cyclophosphamide, (2) medical and maintained with the other physicians caring for the patient history medicine qhs buy cyclophosphamide now, (3) surgical history, (4) social history, including sub to ensure optimal care management. The causes and the effects of the pain Multimodal interventions constitute the use of more than. The literature indicates that the use ately directed neurologic and musculoskeletal evaluation, of multidisciplinary treatment programs compared with con with attention to other systems as indicated. The depression, or anger), psychiatric disorders, personality traits literature is insufficient to evaluate comparisons of multimo or states, and coping mechanisms. Evidence of family, vocational, or legal ment strategy for patients with chronic pain. They also strongly issues and involvement of rehabilitation agencies should be agree that a long-term approach that includes periodic fol noted. The expectations of the patient, significant others, low-up evaluations should be developed and implemented as employer, attorney, and other agencies may also be part of the overall treatment strategy, and that, whenever avail considered. When available, multidis scores are improved over baseline scores for assessment peri ciplinary programs may be used. There is insufficient evidence to establish the effi vidual modalities used in the treatment of chronic pain. A ran botulinum toxin injections, (5) electrical nerve stimulation, domized controlled trial of conventional radiofrequency ab (6) epidural steroids with or without local anesthetics, (7) lation for patients with neck pain and no radiculopathy re intrathecal drug therapies, (8) minimally invasive spinal pro ports pain relief for up to 6 months after the procedure cedures, (9) pharmacologic management, (10) physical or (Category A3 evidence). One randomized controlled trial restorative therapy, (11) psychologic treatment, and (12) comparing water-cooled radiofrequency with sham control trigger point injections. Ablative techniques include the radiofrequency ablation group for up to 3 months (Cat chemical denervation, cryoneurolysis or cryoablation, ther egory A3 evidence). They are equivocal as to whether wa alcohol denervation, with a transient burning sensation as a ter-cooled radiofrequency ablation should be used for reported side effect (Category B3 evidence). Cryoneurolysis or cryoablation: Studies with observational Recommendations for ablative techniques. The Task findings for cryoablation report pain relief for assessment Force notes that other treatment modalities should be at periods ranging from 1 to 12 months among patients with tempted before consideration of the use of ablative lumbar facet joint pain, postthoracotomy neuralgia, or pe techniques. Conventional radiofrequency ablation may be Nerve and nerve root blocks: Studies with observational performed for neck pain, and water-cooled radiofrequency ab findings report that celiac plexus blocks can provide pain lation may be used for chronic sacroiliac joint pain. One randomized controlled tional acupuncture as well as electroacupuncture techniques. Studies with observational randomized controlled trial comparing electroacupuncture findings for medial branch blocks indicate improved pain with conventional acupuncture is equivocal (P 0. Studies with observational findings indicate findings for peripheral nerve blocks indicate effective pain that acupuncture can provide pain relief for assessment peri relief for assessment periods ranging from 1 to 14 days (Cat ods of 1 week to 6 months (Category B2 evidence). Acupuncture may be are equivocal as to whether celiac plexus blocks using local considered as an adjuvant to conventional therapy. Joint blocks: Intraarticular tions compared with facet saline injections regarding pain facet joint injections may be used for symptomatic relief of relief for patients with low back pain (Category C2 evidence). Sacroiliac joint injections may be con However, studies with observational findings for facet joint sidered for symptomatic relief of sacroiliac joint pain. The literature is insufficient to evaluate the treatment of pain secondary to chronic pancreatitis. Lumbar efficacy of sacroiliac joint injections for pain relief (Category sympathetic blocks or stellate ganglion blocks may be used as D evidence). Randomized controlled trials comparing botu linum toxin type A with saline indicate that botulinum toxin ranging from 1 h to 1 month (Category A1 evidence). Subcutaneous should not be used in the routine care of patients with myo peripheral nerve stimulation: Subcutaneous peripheral nerve fascial pain. Botulinum toxin may be used as an adjunct for stimulation may be used in the multimodal treatment of the treatment of piriformis syndrome. Electrical nerve stimula Spinal cord stimulation: Spinal cord stimulation may be tion techniques include neuromodulation with electrical used in the multimodal treatment of persistent radicular pain stimulus. Shared decision making re Neuromodulation with Electrical Stimulus garding spinal cord stimulation should include a specific dis Subcutaneous peripheral nerve stimulation: Studies with ob cussion of potential complications associated with spinal servational findings indicate that subcutaneous peripheral cord stimulator placement. A spinal cord stimulation trial nerve stimulation can provide pain relief for assessment pe should be performed before considering permanent implan riods ranging from 4 months to 2 yr (Category B2 evidence). Reported complications in ulation compared with reoperation (Category A3 evidence). Re domized controlled trials comparing interlaminar epidural ported side effects include insertion-site pain and infections steroids with interlaminar epidural saline are equivocal re (Category B2 evidence). One randomized controlled persistent radicular pain; they all agree that it should be used trial reports lower pain scores at 6 months for leg pain (Cat for other conditions. Similarly, they are equivocal as to whether zi approaches, reports equivocal pain scores for low back pain conotide infusions should be used for refractory chronic pain. In addition, Intrathecal opioid injections: Studies with observational randomized controlled trials are equivocal regarding the ef findings indicate that intrathecal opioid injections can pro ficacy of interlaminar or transforaminal epidural steroids vide effective pain relief for assessment periods ranging from with local anesthetics compared with epidural local anesthet 1 to 12 months for patients with neuropathic pain (Category ics alone for back, leg, or neck pain for assessment periods B2 evidence). They all strongly agree that image guidance lytic blocks: Intrathecal neurolytic blocks should not be per. Intrathecal opioid injections: Intrathecal opioid injection Shared decision making regarding epidural steroid injections or infusion may be used for patients with neuropathic pain. Neuraxial opioid trials should be formed with appropriate image guidance to confirm correct performed before considering permanent implantation of needle position and spread of contrast before injecting a ther intrathecal drug delivery systems. Studies with observational findings indicate that the efficacy of intrathecal neurolytic blocks for pain relief in vertebroplasty and kyphoplasty provide effective relief for chronic non-cancer pain (Category D evidence). In strongly disagree that intrathecal neurolytic blocks should be addition, studies with observational findings indicate that performed for routine care. One randomized trial was should be performed for pain related to vertebral compres equivocal (P 0. An observational study indicates that zi Recommendations for minimally invasive spinal procedures. Randomized controlled trials indicate that somnolence or sedation as reported side effects (Category A1 tramadol provides effective pain relief for assessment periods evidence). In addition, meta-analyses of randomized con ranging from 4 to 6 weeks (Category A2 evidence). A meta periods ranging from 2 weeks to 3 months (Category B2 analysis of randomized placebo-controlled trials is equivocal evidence). Dizziness, somnolence, and pruritus are among regarding the efficacy of selective serotonin reuptake inhibi tors in providing effective pain relief for diabetic neuropathy reported side effects associated with opioid therapy (Category (Category C1 evidence). Selective serotonin reuptake inhibitors may be consid to evaluate the efficacy of trigger point injections. Studies with observational findings suggest that neuropathic or back pain patients, and transdermal, sublin trigger point injections may provide relief for patients with gual, and immediate-release oral opioids may be used. Trigger A strategy for monitoring and managing side effects, ad point injections may be considered for treatment of patients verse effects, and compliance should be in place before pre with myofascial pain as part of a multimodal approach to scribing any long-term pharmacologic therapy. Randomized con trolled trials combining a variety of physical or restorative ther Reference apies. American Society of Anesthesiologists: Practice guidelines for chronic pain management. Similarly, they strongly Appendix 1: Summary of Recommendations agree that physical or restorative therapy should be used for I. Discount cyclophosphamide 50mg with visa. Islamabad: PIMS Confirms 17 Patients With Swine Flu Symptoms.
Elastin fibers intersperse the lamellae and may play an important role in restoration of shape after bending of the spine [161] symptoms endometriosis purchase 50mg cyclophosphamide free shipping. The cellular part of theanulusfibrosusconsistsofthinandelongatedfibroblast-like cells aligned to the collagen fibers (Fig treatment quinsy buy 50 mg cyclophosphamide fast delivery. Surroundedbytheanulusfibrosusisthenucleuspulposus medications in mexico buy cyclophosphamide,thegelatinous core the nucleus is the gelatinous of the intervertebral disc medications known to cause weight gain buy cyclophosphamide 50 mg on-line. The matrix of the nucleus pulposus consists of ran core of the disc and is rich in domly organized collagen fibers and radially arranged elastin fibers that are proteoglycan embedded in a highly hydrated aggrecan-containing proteoglycan gel. Inter spersed at a low density are rounded chondrocyte-like cells usually located inside a capsule in the surrounding matrix (so-called lacunae) [82]. Macroscopically, the boundary between the anulus fibrosus and the gelatinous nucleus pulposus can only be distinguished in young individuals (Fig. The dif ferent mechanical properties of anulus fibrosus and nucleus pulposus are deter mined by composition and organization of the respective extracellular matrix. Although the mechanical properties of nucleus pulposus and anulus fibrosus are very different, the main components are very similar and consist of: water proteoglycans collagen Water makes up 80% of the wet weight of the nucleus and 70% of the wet weight of the anulus [105, 162]. Normal anatomy and composition a Mid-sagittal section through a healthy young intervertebral disc. The white cartilage endplates, the gel-like nucleus pulposus and the surrounding anulus fibrosus can easily be distinguished. Small arrows indicate dissipation of the compressive forces to the anulus fibrosus. On the other hand, the nucleus pulposus that is responsible for dissipat ing the compressive forces on the disc by exerting a hydrostatic pressure on the anulus fibrosus consists of up to 50% of proteoglycans (percent wet weight), whereas the anulus fibrosus only contains 20% proteoglycans (Fig. These differences in proteoglycan content are also reflected by the water content of the two tissues (80% in the nucleus pulposus and 70% in the anulus fibrosus). The exact role of these additional matrix proteins and glycoproteins is not completely clear [55, 87]. It is important to keep in mind that the disc matrix is not a static but a dynamic In the normal disc, matrix structure. The components of the matrix are continuously degraded and degradation and synthesis replaced by newly synthesized molecules. The balance between synthesis, degradation and accumulation of matrix molecules determines the quality and integrity of the disc matrix and is also prerequisite for adaptation/ alteration of the matrix properties to changing environmental conditions. The blood vessels closest to waste removal entirely thediscmatrixarethereforethecapillarybedsoftheadjacentvertebralbodies depend on diffusion and small capillaries in the outermost part of the anulus fibrosus [24, 46]. The blood vessels present in the longitudinal ligaments running adjacent to the disc and in young cartilage endplates (less than 12 months old) are branches of the spinal artery [49, 50, 142]. As a consequence of the avascularity, the nutrient sup ply to the disc cells and removal of metabolic waste products is entirely depen dent on diffusion mainly from or to the capillary beds of the adjacent vertebrae [49]. Animal experiments indicated that the role of the peripheral small capillar ies for the nutrient supply is only of minor importance [102]. The dependency of nutrient supply to the inner parts of the disc on diffusion together with the poor diffusion capacity of the disc matrix severely limits nutrient and waste exchange. As a result, a gradient between the inner parts and the peripheral regions of the disc builds up with very low levels of glucose and oxygen and high levels of the waste product lactic acid on the inside [49] (Fig. These gradients are even fur ther aggravated by the disc cells using oxygen and glucose and producing lactic acid [49, 56]. The restricted nutrient supply and the increasing acidic milieu,due to the accumulation of lactic acid, are considered the main factors limiting cell viability and therefore the integrity of the disc matrix. Macroscopic Disc Alterations Onset and progression of age-related alterations of the disc can be determined with various techniques. Applying this technique revealed that early signs of age-related alterations could Figure 3. Disc nutrition Glucose and oxygen concentration were found to drop steeply from the endplate towards the inner part of the nucleus pulposus (glc glucose, O2 oxygen). Lactate concentration displayed the opposite course, with highest levels in the inner region (laclactate). This profile reflects thenutrient limitations in theinnerdiscandthelowerpH valuesontheinside due to the acidic waste product lactate. The sagittal section through an intervertebral disc shows the region of the deter mined concentrations (adapted from [143]). However, more detailed Disc degeneration starts as information has been gained from macroscopic postmortem analysis of interver early as the second decade tebral disc tissue from individuals of various ages [92]. These studies have led to of life grading systems that on one hand allow the evaluation of stages of disc degenera tion, but also illustrate the process of age-related degeneration. The original grading system was established by Friberg and Hirsch (and propagated by Nach emson) and has been further refined by Thompson et al. Studying age-related changes at the microscopic level, several hall 100 Section Basic Science a c Figure 5. Intervertebral Disc chondrocyte proliferation (increasing cell clusters due to reactive prolifera tion) mucous degeneration (accumulation of mucous substances) cell death tear and cleft formation granular changes: increasing accumulation of granular tissue Cartilage Endplate cell proliferation cartilage disorganization presence of cracks in the cartilage presence of microfractures formation of new bone bony sclerosis First signs of tissue degradation are seen between 10 and 16 years of age when Chondrocyte proliferation tearsinthenucleuspulposusoccuralongwithfocaldisc cell proliferation and is the first sign of disc granular matrix transformation [17]. In parallel, the amount and extent of acidic degeneration mucopolysaccharides in the matrix increase. The general structure of the nucleus pulposus and the anulus fibrosus, however, is preserved in this age group. The nucleusisaccordinglytransformedbymultiple large clefts and tears and the matrix shows significant granular changes. In this age group particularly the anulus fibrosus 102 Section Basic Science Advanceddiscdegeneration is more and more affected, resulting in a loss of the clear distinction between is indicated by a loss of nucleus and anulus. Huge clusters of proliferating cells are observed near clefts and tears that are filled with granular material. In individuals older than 70 years, thestructuralabnormalitieschangemoretoscar-liketissueandlargetissue defects. The histological approach, although it largely parallels the macroscopic classi fication proposed by Thompson et al. Whereas macro a spatial heterogeneity scopic and histological approaches concur in the progressive loss of structure in all anatomical regions of the intervertebral disc, the microscopic approach revealed an earlier occurrence of nuclear clefts already in the second decade of life. In addition, the histologic approach revealed the heterogeneity of the alter ation within the disc, indicating relevant spatial differences with more alter ations usually present in the posterolateral aspects of the disc. In addition, the microscopic approach underlined the importance of nutritional supply to the disc cells for the maintenance of a healthy disc and the lack thereof for the onset and progression of disc degeneration. Since vascularization was seen to disappear from the disc during the first decade, nutritional supply to the disc cells becomes severely impaired during the subsequent phase of growth [17]. Age-Related Changes in Vascularization and Innervation Although there is still some debate over the presence of blood vessels and nerve the disc is the largest endings in the inner portions of pathologic discs, there is consensus that the avascular structure healthy adult disc is the largest avascular and aneural tissue in the human body of the human body [61, 88]. This absence of significant vascular supply to the intervertebral disc matrix has important consequences for the maintenance of discal structures as discussed above [17, 88]. In fetal and early infantile intervertebral discs blood vessels penetrate both the endplate and the peripheral region of the anulus fibrosus. However, by late child hood the blood vessels disappear, leaving only small capillaries accompanied by lymph vessels that penetrate up to 2 mm into the outer anulus fibrosus [46, 124]. Since the importance of this peripheral vascularization for the nutrient supply of the disc is not known in detail, the consequences of its disappearance are also unknown. More important for the blood supply to the inner regions of the disc and therefore better described is the vascularization of the interface between adjacent vertebral bodies, cartilage endplate and the disc. The vertebral bodies are supplied by different arteries that are either responsible for the outer regions, the mid-anulus Vascular changes in the region, or the central core [23, 116]. Co n g e n it a l d e fe ct in ve r t e b r a l a r ch e s w it h cy s t ic d is t e n s io n o f m e n in ge s treatment of tuberculosis discount 50 mg cyclophosphamide with mastercard, b u t n o abnormality of neural tissue symptoms 5dpo order 50 mg cyclophosphamide amex. Co n ge n it a l d e fe c t in ve r t e b r a l a r ch e s w it h c y s t ic d ila t a t io n o f m e n in ge s a n d structural or functional abnormality of spinal cord or cauda equina medications prescribed for migraines cheap cyclophosphamide 50mg on line. Th e d e fe ct m ay b e p a lp a b le symptoms 9 days past iui purchase cyclophosphamide online now, a n d t h e r e m ay b e o ve r lyin g cu t a n e o u s m a n ife s t at io n s (in Ta b le 1 6. Often an in ciden tal fin din g, usually of n o clin ical im por tan ce when it occurs alone. When symptomatic from one of these associated conditions, the presentation is usually that of tethered cord; gait disturbance, leg weakness and atrophy, urinary disturbance, foot deform ities, see Teth ered cord syn d rom e (p. Incidence may increase in times of 6 war, famine or economic disasters, but it may be gradually declining overall. Tr a n s m i s s i o n fo l l o w s non-Mendelian genetics, and is probably multifactorial. The allergy is thought to arise from early and frequent exposure to latex products during medical care for these patients, and there is a suggestion that latex-free surgery on these infants may reduce the risk of the development of latex 8 allergy. Prenatal diagnosis Se e Pre n at a l d e the ct ion of n e u ral t u b e d efe ct s (p. Ge n e r a l m a n a g e m e n t As s e s s m e n t a n d m a n a g e m e n t o f le s io n measure size ofdefect assess whether lesion is ruptured or unruptured 0 ruptured: start antibiotics. Patient is positioned prone, head turned to right (to expose the right occiput), right knee and thigh flexed to expose right flank (con sider using left flank to prevent confusion with appendectomy scar later in life). Su rg ica l t e ch n iq u e o f m yelo m e n in g o ce le re p a ir Ke y c o n c e p t s critical goals: 1) free placode from dura (to avoid tethering), 2) water-tight dural closure, 3) skin clo sure (can be accomplished in essentially all cases). Use latex-free environment (reduces development of latex allergy, as well as attack by maternal antibodies that may have crossed through the placenta). Do not allow scrub solutions or chemical antimicrobials to contact neural placode. Multiple layer closure is advocated, 5 layers should be attempted, although occasionally only 2 or so layers may be closed. There is no evidence that multiple layer closure either improves neurologic function or preven ts later tethering, but there is a suggestion that w hen tethering does occur, it m ay be easier to release when a previous multilayered closure was performed. Silastic does not prevent adherence in series with long follow-up (>6 yrs), and may even render untethering procedures more di cult. Be g in b y d iv id in g t h e a b n o r m a l e p it h e lia l cove r in g fr o m t h e n o r m a l sk in. The dura can then be isolated around the periphery and followed deep to the spinal canal superiorly. The dura is then also for m e d in t o a t u b e an d ap p roxim ate d in a w at er-t igh t closu re. If t h e d u ra can n ot be close d, t h e p la code may be judiciously trim med. Derm oid tum ors m ay result from retained skin during the closure, but alternatively dermoids may also be present congenitally. The most common cause of early mortality are complications from the Chiari malformation (respiratory arrest, aspiration), where late mortal ity is usually due to shunt m alfunction. Six form s are described, the following 3 are clinically impor tant as possible causes of progressive neurologic dysfunction via tethering (p. Th e in t r a d u r a l fa t t y t u m o r m ay a ls o b e k n o w n a s lip o m a o f t h e ca u d a e q u in a. In a d d it io n t o b e in g abnormally low, the conus medullaris is split in the midline dorsally usually at the same level as the 19 bifid spine, and this dorsal myeloschisis may extend superiorly under intact spinal arches. Th e r e is a thick fibrovascular band that joins the lamina of the most cephalic vertebrae with the bifid lamina. Th is b a n d co n st r ict s t h e m e n in go ce le sa c a n d n e u r a l t is su e, ca u s in g a k in k in t h e su p e r io r s u r fa ce o f the meningocele. Th e d u r a is d e h isce n t a t t h e le ve l o f t h e d o r s a l m yelo s ch is is, a n d r e fle ct s o n t o t h e p la co d. Th e lipom a passes through this dehiscence to become attached to the dorsal surface of the placode, and may continue cephalad under intact arches with the possibility of extension into the central canal superiorly to levels without dorsal myeloschisis. The lipoma is distinct from the normal epidural fat which is looser and more areolar. Present at ion In a p e d iat r ic se r ie s, 56%p re se n the d w it h a back m ass, 32%w it h blad d e r p roblem s, an d 10% becau se 22 of foot deformities, paralysis or leg pain. Physical exam inat ion Alm o st a ll p a t ie n t s h a ve cu t a n e o u s st igm a t a o f t h e a s so cia t e d sp in a b ifid a: fa t t y s u b cu t a n e o u s p a d s (located over the m idline and usually extends asym m etrically to one side) w ith or w ithout dim ples, 23 port-wine stains, abnormal hair, dermal sinus opening, or skin appendages. Th e n e u r o lo gic e x a m m ay b e n o r m a l in u p t o 5 0 % o f p a t ie n t s (m o st p r e s e n t in g w it h sk in le s io n only). Present in alm ost all by definition, but 16 some may have segmentation anomalies instead such as butterfly vertebra (p. All p a t ie n t s sh o u ld h ave p r e o p u r o lo g ica l e va lu a t io n t o d o cu m e n t a n y d e ficit. Tr e a t m e n t Sin ce s ym p t o m s a r e d u e t o (1) t e t h e r in g o f t h e sp in a l co rd, e sp e cia lly d u r in g gr ow t h sp u r t s, a n d (2) compression due to progressive deposition of fat, especially during periods of rapid weight gain; the goals of surgery are to release the tethering and reduce the bulk of fatty tumor. Simple cosmetic treatment of the subcutaneous fat pad does not prevent neurologic deficit, and may make later definitive repair more di cult or im possible. Su r gical t r e at m e n t is in d icat e d w h e n t h e p at ie n t r e ach es 2 m on t h s of a ge, or at t h e t im e of d iag nosis if the patient presents later in life. Superior extension along dorsal surface of cord or into central canal is debulked as much as is safely possible 10. Usu a lly lo ca t e d a t e it h e r e n d o f n e u r a l tube: cephalic or caudal. Probably results from failure of the cutaneous ectoderm to separate from the neuro-ectoderm at the tim e of closure of the neural groove. Th e sin u s m ay t e r m in at e su p e r ficia lly, m ay co n n e ct w it h t h e co ccyx, o r m ay t r ave r se b e t w e e n normal vertebrae or through bifid spines to the dural tube. It may widen at any point along its path to form a cyst; called an epidermoid cyst if lined with stratified squamous epithelium and contain ing only keratin from desquam ated epithelium, or called a derm oid cyst if also lined w ith derm is (containing skin appendages, such as hair follicles and sebaceous glands) and also containing sebum and hair. Alt h o u gh in n o cu o u s in a p p e a r a n ce, t h e y a r e a p ot e n t ia l p a t h w ay for in t r a d u r a l in fe ct io n w h ich may result in meningitis (sometimes recurrent) and/or intrathecalabscess. The lining dermis contains normal skin appendages which may result in hair, sebum, desquamated epithelium and cholesterol, within the tract. As a result, the contents of the sinus tract are irritating and can cause a sterile (chemical) meningitis with possible delayed arachnoiditis if it enters the dural space. In cid en ce of a p resu m ed sacral sin u s (a d im ple w h ose bot t om cou ld n ot be see n on skin re t rac tion): 1. If t h e t ract expan d s in t rat h ecally t o form a cyst, t h e m ass m ay p resen t as a t et h ered cord or as an intradural tum or. Th e t r a ct fr o m a sp in a l d e r m a l sin u s a lw ays co u r se s ce p h a la d a s it d ive s in w a r d fr o m t h e su r fa ce. An o ccip it a l s in u s m ay p e n e t r a t e t h e sk u ll a n d ca n co m m u n ica t e w it h d e r m o id cyst s a s d e e p a s t h e cerebellum or fourth ventricle. Ra d io lo g ic e va lu a t io n When seen at birth, ultrasound is the best m eans to evaluate for spina bifida and a possible m ass inside the canal. Plain x-rays m ust be done w hen em barking on surgery as part of operative planning, as prepara tion for the possibility of a complete laminectomy. Tr e a t m e n t Sin u s e s a b ove t h e lu m b o sa cr a l r e gio n sh o u ld b e s u r gica lly r e m ove d. Although 25%of presumed sacral sinuses seen at birth will regress to a deep dimple on follow-up (time not specified), it is recommended that all dermal sinuses should be surgically explored and fully excised prior to the development of neurologic deficit or signs of infec tion. |