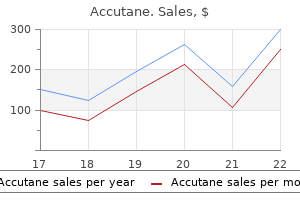
Alita Loveless, MD
The risk may be affected by studies acne hat accutane 30 mg generic, caffeine was given in the form of tablets1 skin care trade shows cheap accutane 40mg fast delivery,2 or as 2 to 7 cups individual susceptibility acne 9gag order cheap accutane on-line, the additive stimulant effects of caffeine acne 4 week old baby buy accutane without a prescription, of instant coffee. Because of the quality of the clinical evidence (controlled the authors of one report1 advised that users of phenylpropanol pharmacokinetic studies), experimental data have not been sought. C amine should be warned about the over-use of phenylpropanol amine, and also about taking caffeine at the same time, because of the possible risk of intracranial haemorrhage secondary to severe hypertension. If both drugs are given the probable mechanism of the interaction is that the two drugs there is the potential for increased caffeine adverse effects (such as compete for the same metabolic route resulting in a reduction in their headache, jitteriness, restlessness and insomnia). Transient hypertension after two phenylpropanolamine diet aids and the effects of caffeine: a placebo-controlled follow up study. Adverse drug effects attributed to such as coffee, tea, cola drinks, or medications, etc. Influence of usual intake of dietary caffeine on single-dose kinetics of theophylline in healthy human subjects. Calamus is traditionally used as a carminative and spasmolytic, in acute and chronic Constituents dyspepsia, gastritis and gastric ulcer, intestinal colic and the main active constituents are found in the volatile oil, but anorexia, and for respiratory disorders. Tetraploid Pharmacokinetics (subtropical, specifically Indian) species contain 96% No relevant pharmacokinetic data found. Flavonoids (specifically flavonol glycosides including isoquercitrin, narcissin, neohesperidoside and rutin) have also been identified. For information on the interactions of individual flavonoids present in calendula, Calendula is often used in externally applied products for the see under flavonoids, page 186. Dose-linear pharmacokinetics of oleanolic acid after intravenous and oral administration duodenal ulcers, haemorrhoids and varicose veins. When smoked, cannabinoid acids are decar boxylated by the high temperature, and reach the lung as active free cannabinoids. Psychotropic effects start from Constituents within seconds to a few minutes, reach a maximum after 20 Cannabis herb contains a wide range of cannabinoids, which to 30 minutes, and taper off within 3 to 4 hours. However, other 90 minutes, reaching their maximum after 2 to 4 hours and cannabinoids, which do not possess psychoactive properties, lasting for about 6 hours. The cannabinoids are mene, are increasingly being investigated for their pharma extensively metabolised by cytochrome P450, in particular, cological and therapeutic properties. However, medicinal cannabis is increasingly being used to Interactions overview treat chronic conditions, as an adjunct, or where other Most of the drug interaction data relate to smoking cannabis. For example, a buccal spray Smoking cannabis has been shown to decrease levels of preparation of cannabis, containing mainly dronabinol (the 9 theophylline, chlorpromazine and probably clozapine. Tachycardia tomatic relief of neuropathic pain in multiple sclerosis in has also been seen with combined use of tricyclic adults. It is also being investigated for use as an analgesic in antidepressants and cannabis. Cannabis might increase the other disease states such as diabetic neuropathy and effects of opioids such as morphine. Isolated cases of rheumatoid arthritis, and to relieve spasticity in multiple hypomania have been seen when cannabis was used with sclerosis and spinal cord injury. Dronabinol and nabilone (a disulfiram and with fluoxetine, and a man taking cannabis synthetic cannabinol) are used as antiemetics in patients and sildenafil had a myocardial infarction. Indometacin might antagon used illicit drug because of its psychoactive properties, and ise some of the effects of smoking cannabis. Smoking has a long history of such use, including by those with cannabis does not appear to affect the pharmacokinetics or chronic illnesses. Cytochrome P450 107 108 Cannabis enzymesinvolved in themetabolismof tetrahydrocannabinols andcannabinol by human Randomized, double-blind, placebo-controlled study about the effects of cannabidiol9 hepatic microsomes. Characterization of P-glycoprotein inhibition by major cannabinoids from marijuana. Narcotic drugs change the expression of cytochrome P450 2E1 and 2C6 Pharmacol Exp Ther (2006) 317, 850?7. The effects of cannabinoids on P-glycoprotein transport and expression in multidrug 5. C Cannabis 109 Importance and management Cannabis + Alcohol Several studies have found that cannabis and alcohol produce additive detrimental effects on driving performance, but other the detrimental effects of drinking alcohol and smoking studies have not found any potentiation. This is probably due to the cannabis may be additive on some aspects of driving perform variety of simulated driving tests used and possibly the time lag ance. However, there is some evidence that regular cannabis use between the administration of alcohol and cannabis; behavioural in itself does not potentiate the effects of alcohol. Smoking impairment after cannabis has been reported to peak within 30minutes of smoking. Concurrent use of cannabis and Evidence and mechanism alcohol before driving should therefore be avoided. Marijuana and alcohol combined performance of psychomotor tests, suggesting that those who use severely impede driving performance. AnnEmerg both drugs together should expect the deleterious effects to be Med (2000) 35, 399?400. Divided attention performance in cannabis users and non 70mg%, with further drinks taken to maintain levels at 40mg%) users following alcohol and cannabis separately and in combination. Modulation of the effects of alcohol on driving-related both alcohol and cannabis resulted in dramatic performance psychomotor skills by chronic exposure to cannabis. Psychopharmacology (Berl) impairment as great as that observed with blood-alcohol levels of (2002) 160, 213?19. Acute and residual effects of alcohol and marijuana, alone and in combination,onmoodandperformance. Psychopharmacology(Berl) (1994)115,340? synergistic impairment of performance)4 have been found in a 9. Separate and combined effects of marijuana and 5 alcohol on mood, equilibrium and simulated driving. Cannabis intoxication and fatal cigarettes and drank moderate amounts of alcohol, found that the road crashes in France: population based case-control study. Marihuana number of euphoric events in response to a cannabis cigarette was attenuates the rise in plasma ethanol levels in human subjects. Neuropsychopharma greater after alcohol ingestion, and the duration of euphoric events cology (1992) 7, 77?81. The speed of onset of the effects of cannabis was also faster when it was smoked after the ingestion of alcohol. In this study, neither group had smoked any cannabis in the 12hours before the alcohol test. There were no significant additive effects on brake latency, body sway or mood when the two Clinical evidence drugs were used together. The probable reason is that some of the components plasma alcohol levels were only 55mg% and they occurred of tobacco smoke act as enzyme inducers, which increase the rate at 55minutes later. In addition, their subjective experience of the which the liver metabolises chlorpromazine, thereby reducing its drugs decreased when used together. This interaction is based on experimental stopped smoking both tobacco and cannabis. Irregular smoking of Importance and management cannabis might cause fluctuations in clozapine levels. These data require confirmation in smoking cessation can lead to intoxication with clozapine or olanzapine. Until such data are available, bear in mind the possibility Psychopharmacol (2002) 17, 141?3. Inhibitionof cyclosporineandtetrahydrocannabinol Cannabis + Disulfiram metabolism by cannabidiol in mouse and human microsomes. Two isolated case reports describe hypomanic-like reactions when patients taking disulfiram used cannabis, whereas no unusual interaction with the combination was seen in other subjects. Cannabis + Cisplatin Evidence, mechanism, importance and management A case report describes a fatal stroke when a young man A man with a 10-year history of drug abuse (alcohol, amfetamines, receiving cisplatin smoked cannabis. The patient said that he felt as though he had been taking developed tinnitus and paraesthesias after receiving the first course amfetamine. Exclusion criteria: Pregnancy or nursing women skin care vitamin e generic 10 mg accutane visa, serious general diseases skin care on center purchase 30 mg accutane with visa, psychiatric disturbances acne 10 days before period purchase cheap accutane line, medico-legal litigation acne 24 discount accutane 30 mg with amex. Evaluation was based upon a sum score including both subjective and objective measures. Follow-up: 3 weeks, 2 & 6 months Notes Authors results and conclusions: In subgrp. Funded by: grant from the Centro Studi di Patologia Vertebrale, Rome Principal author is an orthopedist? Unclear risk Note: No other information was provided on the sequence generation or allocation. High risk Patient was not blinded; therefore, this item was All outcomes outcome assessors? No mention if there were any at tempts to blind the outcome assessors to treatment allocation for the subjective or objective outcome measures. High risk 8% (38/459) of the subjects had interrupted or changed their assigned treatment. Low risk Spinal manipulative therapy for chronic low-back pain (Review) 96 Copyright 2011 the Cochrane Collaboration. Exercises (extension): All patients were instructed in 2 simple extension exercises (exten sion-in-lying, and repeated extension-in-standing). The exercises were to be performed 3 to 5 times with a gradual increase of the extension. The patients were instructed to perform these exercises as often as possible during the day and at least once per hour. Follow-up: 2 & 4 weeks, 1 year Notes Authors results and conclusions: Pain in both back and legs decreased without differences betweenthegrps. Noadditionaleffectwasdemonstratedofmanipulationwhenextension exercises were used as a basic therapy. Funding by the Oak Foundation Uncertain what the background is of the primary and co-authors. The information of whether to re ceive manipulation or not was given to the ex Spinal manipulative therapy for chronic low-back pain (Review) 97 Copyright 2011 the Cochrane Collaboration. Rasmussen 2008 (Continued) aminer in an envelope in the medical chart to be opened by the end of the manual medical exam ination, when the patient was lying on the side. The patients were not informed of their therapy (manipulation or not) before the end of the fol low-up, then a letter with a description of the ran domisation was sent to their general practitioner who had referred the patient to the study. Unclear risk Note: no other information was provided regard ing randomisation or allocation. Our resultsdidnotpointtowardssuchbiasastheresults in the manipulated group were no better than in controls. The blindingof the examiner wasfur thermore attempted by mixing patients at differ ent stages of the project? (comment: no statement as to whether the outcome assessor was blinded to treatment allocation). High risk 56 patients responded to the questionnaires after All outcomes drop-outs? High risk Functional status and recovery not reported; no published protocol available Spinal manipulative therapy for chronic low-back pain (Review) 98 Copyright 2011 the Cochrane Collaboration. Low risk Similar for the most important sociodemographic measures, including baseline pain; however, ma nipulation grp. Low risk Regarding exercise: after 4 weeks 100% reported daily exercises, and at one-year follow-up 79% in group A and 75% in group B respectively, re ported to be exercising as instructed several times per week. Baseline values or changes in these were not related to compliance at one-year follow-up. Exclusion criteria: Prior segmental stabilizing training, manual treatment in the previous 3 months, prior spinal surgery, radiation to the leg or legs with overt neurological signs, pregnancy, known lumbar disc hernia, diagnosed in? The patients were taught how to activate the deep abdominal muscles together with relaxed breathing in different positions. The physiotherapist monitored the patient by palpating the lower abdominal quadrant for Spinal manipulative therapy for chronic low-back pain (Review) 99 Copyright 2011 the Cochrane Collaboration. They could include a combination of muscle stretching, segmental traction, and soft tissue mobilization and, if needed mobilization of stiff thoracic and upper lumbar segments. The patients were encouraged to go on with their usual ac tivities or exercises (not controlled). The men and the women were then separately and consis tently randomised to either group. Unclear risk Unclear to what extent the physiotherapist was in volved in the treatment allocation; no mention of an independent research assistant involved in this aspect; thus, unclear what safeguards were in place to protect sequence generation. Spinal manipulative therapy for chronic low-back pain (Review) 100 Copyright 2011 the Cochrane Collaboration. Unclear risk Recovery was not reported; no published protocol was available Similarity of baseline characteristics? Unclear risk By design, patients were not allowed the interven tion in which they were not randomised; patients were queried at 3 & 12 months regarding whether they had sought additional physiotherapy follow ing the last therapy session; however, the authors do not report whether other interventions were sought during or following the treatment phase. Low risk Spinal manipulative therapy for chronic low-back pain (Review) 101 Copyright 2011 the Cochrane Collaboration. Exclusion criteria: Symptoms too mild as determined by an administrator, pregnancy, speci? Preventive and rehabilitating advices on physical activity and ergonomics were often given. The evidence-based care was given in direct conjunction with the medical examination (an additional 15 min). A booklet with examples of exercises and general information on back and neck pain was provided. Secondary outcomes: perceived recovery (based upon an 11 point scale) and subsequently dichotomized. Skillgate 2007 (Continued) to minor short-term reactions such as muscle soreness, tiredness, and increased pain, typically following the? This trial suggests that combined manual therapy, like naprapathy, might be an alternative to consider for back and neck pain patients. Funding: Swedish Research Council, the Stockholm County Council, the Uppsala County Council, Capio; the Swedish Naprapathic Association and Health Care Science Post-Graduate School at Karolinska Institute. Long-term data (1 year) to be available in a 2010 publication (not published at the time of this review). Low risk Included patients were assigned to 2 groups by randomisation and no pre strati? An assistant not involved in the project prepared 500 opaque, sequentially num bered sealed envelops with cards numbered 1 or 2 (randomised by a computer), indicating the 2 interventions. Patients were sequentially num bered in the order they came to the study center and received the assignment envelope with the corresponding number. Low risk the unmasking was performed by the physician after the medical examination, so that the assis tant, the physician, and the patient were all blind to the group assignment until after all patient baseline data were collected. All outcomes in the trial were self-rated by web-based or postal questionnaire 5 times during the year following Spinal manipulative therapy for chronic low-back pain (Review) 103 Copyright 2011 the Cochrane Collaboration. Low risk Follow-up (% retained) at 3 weeks: Naprapathy All outcomes drop-outs? Unclear risk the treatments in both groups were conformed to the patients? condition, but standardized as far as possible concerning, for example, the length of treatment sessions and how to perform them in different situations, by several group meet ings held in advance with the physicians and the naprapaths. Spinal manipulative therapy for chronic low-back pain (Review) 104 Copyright 2011 the Cochrane Collaboration. Exclusion criteria: Patients were not eligible if: They were aged 65 or over, because the spinal manipulation package could be more hazardous in older people with osteoporo sis; there was a possibility of serious spinal disorder, including malignancy, osteoporosis, ankylosing spondylitis, cauda equina compression, and infection; complained mainly of pain below the knee, as clinical outcome was likely to be different; had previously had spinal surgery, as clinical outcome was likely to be very different; had another mus culoskeletal disorder that was more troublesome than their back pain; had previously attended, or been referred to , a specialised pain management clinic; had a severe psychi atric or psychological disorder; had another medical condition, such as cardiovascular disease, that could interfere with therapy; had moderate to severe hypertension (systolic blood pressure > 180 mm Hg or diastolic blood pressure > 105 mm Hg, on at least two separate occasions; were taking anticoagulant treatment; were taking long term steroids, which might lead to osteoporosis; could not walk 100 m when free of back pain, because exercise would be dif? Clinical and support staff from the participating practices were invited to training sessions on the active man agement? of back pain. Copies of The Back Book? were provided as well as the corre sponding patient booklet. It comprises ini tial individual assessment followed by group classes incorporating cognitive behavioural principles. We invited participants to attend up to eight 60 minute sessions over four to eight weeks and a refresher? class 12 weeks after randomisation. The three professional associations agreed to the use of this package in this trial. They all had a minimum of two years? clinical experience and were skilled in a range of manipulative techniques, including high velocity thrusts. Participants randomised to private manipulation received treatment in manipulators? own consultation rooms. Order accutane 5 mg fast delivery. Frequently Asked Questions About Microdermabrasion - Lebo Skin Care.
Because such a nonlinearity causes increasing orders of operators by commutation [97] skin care vancouver buy cheap accutane on line. So far acne x lactoferrin order accutane, we have seen how to characterize and control the Hilbert space of our linear skin care anti aging order line accutane, 3 skin care 35 year old order 20mg accutane visa. This technique interleaves classical displacements on the resonator with number-selective Berry phases on the qubit. Because the Berry phase is number-selective, resonator Fock states can be interfered by applications of the displacement operator, which can leave the resonator in a highly nonclassical state. For instance, resonator photons can be exchanged with a thermal bath, or the phase of a quantum superposition can be randomized by unitary evolution. The cost of relying on the large Hilbert space of an oscillator is that the sensitivity to these interactions increases rapidly for macroscopic superposition states [11]. Phase noise is treated in a similar manner, introducing a phase scattering process with the bath to compute its e? This allows us to solve for the evolution of the density matrix of the resonator given some spurious process. We can write down a Lindblad equation to describe this evolution of the resonator under this interaction [35] as d? Therefore, T2 T1, even though energy decay is the only decoherence mechanism present! In this case, the interaction with the bath does not exchange resonator photons between the modes (as in the case of energy decay). It turns out that superpositions of coherent states have an interesting consequence for photon-loss mechanisms too [99]. Parity measurements therefore, can act as a photon-loss error detector, without collapsing the state since |? However, the two-legged cat [11] can only encode a classical bit of information (whether the parity is +1 or -1). To encode a quantum bit, each parity subspace needs to contain an entire logical Bloch sphere [99]. One basis that can encode superpositions within a parity subspace are four-legged cats. Because our logical states are chosen in the even parity subspace, all logical states have only even Fock weights [11], as X |? L Detecting any of these error states will indicate that an error has occurred in the memory. To see how errors can be decoded, consider the action of the annihilation operator 3. The Wigner function of the logical states |0iL (blue star) and |1iL are shown for |? However, a second photon loss even leads to an undetected error, since the state is back in the logical basis but at a new point on the logical Bloch sphere. Consequently, our state is never destroyed by photon loss, though the deterministic energy loss still occurs at rate. Although encoding a qubit state onto a four-legged cat has been achieved [68], universal control over a logical cat-qubit, for instance using the techniques in [69], is an important next step for the scheme. Finally, putting all of these pieces together, and showing overall gains in qubit performance, will be an incredible triumph. On their own, res M onators can serve as a test bed for studying material losses [101?104]. Coupled to superconducting qubits, low-loss resonators can act as quantum memories [52, 75, 107] or as buses for exchanging quantum information between qubits [57, 58]. This thesis is primarily concerned with one of these applications in particular, the quantum memory performance of a resonator. Therefore, we begin this chapter by presenting a generalized framework for to describe how loss mechanisms a? With that context, we present the design and development of a suite of low-loss microwave resonators and discuss the challenges and opportunities of a number of resonator geometries. This chapter culminates in the discovery of a viable technique for achieving state-of-the-art quantum memory performance for a superconducting-qubit-coupled device [52]. In practice, all circuit elements have some complex impedance that is neither completely capacitive nor inductive. Further, the concept of electromagnetic resonance is much more general than parallel or series circuits. The second observation that allows us to write down the quantum mechanical description of such a system is the treatment of boundary conditions [14]. Each resonator has a particular set of boundary conditions that forces these wave equations to a set of discrete eigenmodes. A given distribution of electromagnetic energy can be written as a sum over these modes [14], such that X? In reality however, only the Josephson element can usually be treated as a lumped element. The linear part of the Josephson inductance may add another set of eigenmodes to the system and perturb the existing ones, but we can account for this using similar techniques as before [10]. After the linear system has been solved, we only need to know the location of the junction (x = xJ) to? We see in later chapters explicitly how this term is calculated by full 3D simulations. Therefore, the ultimate quantum coherence that a resonator can posses is T2 = 2T1 = 2Q/. If a full circuit model is available, the quality factor can be calculated by 1 Q =, (4. The power dissipated in each of these loss mechanisms combines to make the the total power dissipated in the circuit equal to X? Because the average total energy stored in the resonator is a single quantity, we can write the quality factor as 1 1 X =? Changing geometries while holding all of the materials properties constant will change Qn. For a physical circuit, many loss mechanisms can contribute to the damping of energy in the system. The dissipation of each of these elements adds to the total dissipation rate of the circuit. We can make progress in understanding a given total dissipation rate through experiments which selectively probe one such mechanism, such as conductor loss. This notion is already common for cavity resonators limited by conductor loss, where a geometrical factor G is expressed in Ohms such that the observed quality factors are Q? G/R [111], where R is the sheet resistance of the conductor used to fabricate the resonator. We generalize this notion to generic loss mechanisms next, as participation ratios. Participation ratios are a useful framework for quantifying loss in any device [112]. The idea is to use straightforward accounting to interpret decay rates in a way that educates a circuit designer about the losses in the system. These ratios can lead to surprising conclusions about what limits a given performance [105, 106]. Comparing many variations of one main geometry can test scaling hypotheses about certain loss mechanisms [104]. To accomplish this accounting, we simply re-express Qn to tease apart the geometry 4. The key to designing a low-loss circuit is to know what systems have high qn and store as much of the energy there as possible. Let us look at a few classic loss mechanisms for a superconducting microwave resonator, using the language of participation ratios. Following Schuster [62], the coupling capacitor transforms the real impedance of the load, which we can recast as a parallel admittance as 1 j? Introducing a real impedance to the circuit for control or readout purposes will be associated with some external dissipation. Surface dielectrics, on the other hand, tend to have smaller participation by virtue of their signi? Possible better long-term survival in left versus right-sided colon cancer a systematic review acne 40s accutane 20 mg. Outcome after liver resection in patients presenting with simultaneous hepatopulmonary colorectal metastases skin care natural tips 20 mg accutane otc. Occurrence and survival of synchronous pulmonary metastases in colorectal cancer: a nationwide cohort study skin care companies buy accutane 30 mg lowest price. Effect of specialist decision-making on treatment strategies for colorectal liver metastases skin care 60 effective 5 mg accutane. High-frequency jet ventilation for minimizing breathing-related liver motion during percutaneous radiofrequency ablation of multiple hepatic tumours. Bacterial Culture Prior to administering antibiotics, ascitic fluid (at least 10 mL) should be obtained and then directly inoculated into a blood culture bottle at the bedside, instead of sending the fluid to the laboratory in a syringe or container, since immediate inoculation improves the yield on bacterial culture from approximately 65 to 90%, 3 9 when the ascitic fluid cell count is at least 250 cells/mm (0. Laboratory diagnostic criteria for secondary bacterial peritonitis includes at least two of the following: ascitic fluid protein greater than 1 g/dL, lactate dehydrogenase higher than the upper limit of normal for serum, or glucose less than 50 mg/dL. These tests can be submitted to the laboratory using a red-top tube and may include albumin, total protein, glucose, lactate dehydrogenase, amylase, and bilirubin. Biliary leakage into the peritoneum can be associated with increased ascitic fluid bilirubin concentration. For patients with a prior paracentesis, especially a recent paracentesis, most of these additional diagnostic tests will not need repeating. Indeed, patients with culture-negative neutrocytic ascites have similar mortality rates as patients with confirmed spontaneous bacterial peritonitis and benefit from antibiotic treatment, which should not be delayed while awaiting bacterial culture results (Figure 2). Any cirrhotic patient with a positive ascitic fluid culture who has concerning signs or symptoms that may indicate infection, such as fever (temperature greater than 37. Extended spectrum antibiotics, such as carbapenems, may even be considered in nosocomial cases. The choice of treatment will depend on location of acquisition (community versus nosocomial), local resistance patterns, and culture sensitivity results when available. Use of intravenous albumin should be reserved for patients with a serum creatinine greater than 1 mg/dL, blood urea nitrogen greater than 30 mg/dL, or total bilirubin greater than 4 mg/dL. Patients with secondary bacterial peritonitis should undergo surgical intervention of the perforated viscus or drainage of the abscess and should be treated with broad-spectrum antibiotics, such as third-generation cephalosporins, with the addition of an antimicrobial agent that has good anaerobic coverage, such as metronidazole. In one metaanalysis of five trials, antibiotic prophylaxis in cirrhotic patients with gastrointestinal bleeding demonstrated a 9% increase in survival. If intravenous ceftriaxone cannot be used due to a severe beta-lactam allergy, intravenous ciprofloxacin 400 mg every 12 hours could be used as the initial prophylaxis regimen during active bleeding. Ascitic fluid should be sent for cell count and differential analysis and should be directly inoculated into blood culture bottles at the bedside. Daily dosing is preferred over intermittent dosing due to the increased risk of developing antimicrobial resistance with intermittent dosing. For patients with acute gastrointestinal hemorrhage, intravenous ceftriaxone 1 g daily is recommended for a total duration of 7 days and has been shown to decrease the risk of infections, re bleeding, and mortality. Alternatively, once patients are stable with control of bleeding and resumption of oral intake, the ceftriaxone may be transitioned to oral ciprofloxacin 500 mg twice daily to complete the 7-day course. Review article: spontaneous bacterial peritonitis-bacteriology, diagnosis, treatment, risk factors and prevention. Prevalence of peritonitis and the ascitic fluid protein concentration among chronic liver disease patients. Intestinal permeability in cirrhotic patients with and without spontaneous bacterial peritonitis: is the ring closed? Translocation of gut bacteria in rats with cirrhosis to mesenteric lymph nodes partially explains the pathogenesis of spontaneous bacterial peritonitis. Microbiology and resistance in first episodes of spontaneous bacterial peritonitis: implications for management and prognosis. A Real-World Evaluation of Repeat Paracentesis guided Management of Spontaneous Bacterial Peritonitis. Risk factors for spontaneous bacterial peritonitis in cirrhotic patients with ascites. Incidence and predictive factors of first episode of spontaneous bacterial peritonitis in cirrhosis with ascites: relevance of ascitic fluid protein concentration. Low-protein-concentration ascitic fluid is predisposed to spontaneous bacterial peritonitis. Recurrence of spontaneous bacterial peritonitis in cirrhosis: frequency and predictive factors. Systematic review and meta-analysis of the possible association between pharmacological gastric acid suppression and spontaneous bacterial peritonitis. Bacterial infection in patients with advanced cirrhosis: a multicentre prospective study. Lack of increased bleeding after paracentesis and thoracentesis in patients with mild coagulation abnormalities. Culture-negative neutrocytic ascites: a variant of spontaneous bacterial peritonitis. Bedside inoculation of blood culture bottles is superior to delayed inoculation in the detection of spontaneous bacterial peritonitis. Secondary bacterial peritonitis in cirrhosis: a retrospective study of clinical and analytical characteristics, diagnosis and management. Utility of an algorithm in differentiating spontaneous from secondary bacterial peritonitis. Clarification of risk factors for abdominal operations in patients with hepatic cirrhosis. Ascitic fluid carcinoembryonic antigen and alkaline phosphatase levels for the differentiation of primary from secondary bacterial peritonitis with intestinal perforation. Infected ascites: Distinguishing secondary peritonitis from spontaneous bacterial peritonitis in a cirrhotic patient with classic symptoms. Two different dosages of cefotaxime in the treatment of spontaneous bacterial peritonitis in cirrhosis: results of a prospective, randomized, multicenter study. Cefotaxime is more effective than is ampicillin-tobramycin in cirrhotics with severe infections. Randomized, comparative study of oral ofloxacin versus intravenous cefotaxime in spontaneous bacterial peritonitis. Short-course versus long-course antibiotic treatment of spontaneous bacterial peritonitis: a randomized controlled trial of 100 patients. Ceftriaxone in the treatment of spontaneous bacterial peritonitis: ascitic fluid polymorphonuclear count response and short-term prognosis. Long-term prognosis of cirrhosis after spontaneous bacterial peritonitis treated with ceftriaxone. Five days of ceftriaxone to treat spontaneous bacterial peritonitis in cirrhotic patients. Five days of ceftriaxone to treat culture negative neutrocytic ascites in cirrhotic patients. Oral ciprofloxacin after a short course of intravenous ciprofloxacin in the treatment of spontaneous bacterial peritonitis: results of a multicenter, randomized study. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. Primary prophylaxis of spontaneous bacterial peritonitis delays Page 11/19 hepatorenal syndrome and improves survival in cirrhosis. Risk factors for the development of bacterial infections in hospitalized patients with cirrhosis. Antibiotic prophylaxis for the prevention of bacterial infections in cirrhotic patients with gastrointestinal bleeding: a meta-analysis. Improved survival after variceal bleeding in patients with cirrhosis over the past two decades. Norfloxacin prevents spontaneous bacterial peritonitis recurrence in cirrhosis: results of a double-blind, placebo-controlled trial. Trimethoprim-sulfamethoxazole for the prevention of spontaneous bacterial peritonitis in cirrhosis: a randomized trial. Ciprofloxacin and long-term prevention of spontaneous bacterial peritonitis: results of a prospective controlled trial. Epidemiology of severe hospital acquired infections in patients with liver cirrhosis: effect of long-term administration of norfloxacin. Norfloxacin vs ceftriaxone in the prophylaxis of infections in patients with advanced cirrhosis and hemorrhage. |