Jeremy Greene, M.A., M.D., Ph.D.
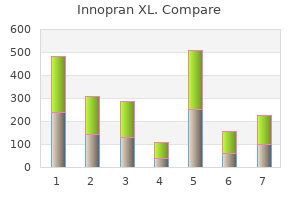
 https://www.hopkinsmedicine.org/profiles/results/directory/profile/9622265/jeremy-greene Although the long-term risks and benefits of hydroxyurea are not known blood pressure chart for 14 year old purchase innopran xl 80 mg fast delivery, current clinical experience has not identified any clear detrimental effects or safety concerns prehypertension 21 years old purchase genuine innopran xl on line. The pain has persisted despite minimal activity since that time blood pressure medication side effects cough discount innopran xl 40 mg fast delivery, and the pain has not been relieved with the use of ibuprofen heart attack female generic innopran xl 80mg visa. He has been seen in your office since he was an infant, and he has no history of any medical problems. He has been doing well in school and had been active in sports before this injury, with no history of prior leg injuries. Radiographs reveal a lytic bone lesion in the distal left femur, with no fracture. The differential diagnosis of painful bony lesions in children includes all of the following except (A) osteosarcoma (B) Ewing sarcoma (C) osteoid osteoma (D) nonossifying fibroma (E) osteomyelitis 2. Which of the following sites within bones is the most common primary site for osteosarcoma Which of the following is the peak age range for diagnosis of patients with Ewing sarcoma Which of the following clinical features is least likely to distinguish osteosarcoma from Ewing sarcoma Which of the following is not a clinical feature of Langerhans cell histiocytosis Which of the following is the least likely laboratory finding in patients with hemophagocytic lymphohistiocytosis Which of the following blood products should not be used in pediatric patients with malignancies who are receiving chemotherapy In which of the following clinical situations is a platelet transfusion least likely to be effective Which of the following microorganisms cannot be acquired via blood product transfusions Features of patient reactions to red blood cell transfusions include all of the following except (A) temperature higher than 101. Long-term complications of radiation therapy include all of the following except (A) diabetes mellitus (B) secondary amenorrhea (C) coronary artery disease (D) restrictive lung disease (E) growth retardation 16. Which of the following types of chemotherapy is not matched correctly with one of its side effects Osteosarcoma (also known as osteogenic sarcoma) is a relatively common pediatric malignancy, with approximately 400 cases per year in children younger than 20 years of age in the United States. They also represent ideal targets for the development of tumor-specific therapeutics. Ewing sarcoma accounts for approximately 100 cases of pediatric malignancy per year in the United States. Osteoid osteoma is a common benign bony lesion that generally occurs in the lower extremities and presents with night time pain that is relieved with nonsteroidal anti-inflammatory medications. Nonossifying fibromas (also called fibrous cortical defects) are benign developmental defects in ossification that are painless, usually only detected incidentally, and require no therapy (see Figure 90-1). The most common sites of osteosarcoma are at those sites with the most rapid bone growth: the distal femur, proximal tibia, and proximal humerus. Approximately 65% of all osteosarcomas occur in the femur, and more than 80% of femoral osteosarcomas occur in the distal end. The second most common site is the proximal tibia; the third most common site is the proximal humerus. In general, the outcomes for localized osteosarcoma are good, with 60-80% long-term survival with current treatments. Children with metastatic osteosarcoma, however, do significantly worse, with only a 20-30% survival rate. Osteosarcoma can also rarely occur in flat bones such as the skull, ribs, and pelvis, where it also has a much poorer outcome. The development of osteosarcoma may in part be associated with the rapid bone growth that occurs during these times. Osteosarcoma is very rare in children younger than 5 years of age and uncommon in adults older than 30 years of age. Children with cases of bilateral retinoblastoma almost always have germ-line mutations in the R b gene, which are also associated with an increased incidence of secondary malignancies, approximately 50% of which are osteosarcomas. The risk of osteosarcoma in patients with Rb gene mutations is approximately 500 times that of the general population. Prior radiation exposure, including radiation therapy for childhood malignancies, is also associated with an increased incidence of osteosarcoma. Radiation exposure has been linked to up to 5% of osteosarcoma cases, and osteosarcoma can occur up to 40 years after exposure to radiation. A family history of sarcomas, leukemias, adrenocortical carcinomas, and breast and bone cancers can be found in families with hereditary mutations in the p53 gene, termed the Li-Fraumeni syndrome, which also is associated with an increased incidence of osteosarcoma. Other syndromes associated with increased osteosarcoma incidence include Paget disease and Ollier disease (enchondromatosis), both of which more commonly are associated with adult-onset osteosarcoma. Approximately 70% of the cases occur in children younger than 20 years of age, and half of the cases occur between 10 and 20 years of age. Ewing sarcomas are also extremely rare in African Americans and Asians, occurring most commonly in white populations. There is no apparent connection between the onset of Ewing sarcoma and the occurrence of puberty, and there are no associated syndromes or exposures that increase the risk of Ewing sarcoma. The primary sites for Ewing sarcoma are the pelvis and lower extremities, with approximately 20% of cases in the pelvis, 20% in the femurs, and 10% each in the tibias and fibulas. Approximately 9% of cases occur in the chest wall and are sometimes known as Askin tumors. Ewing sarcomas are more common in the axial skeleton than osteosarcomas, but approximately 3% of cases occur in the skull. However, Ewing sarcoma and osteosarcoma have distinct features that can assist in the diagnosis before biopsy. Ewing sarcoma tends to be associated with systemic symptoms such as fever and weight loss, whereas osteosarcoma usually presents with local symptoms such as pain and swelling. Ewing tumors are more commonly located in the axial skeleton and are usually diaphyseal, as opposed to osteosarcomas that are more commonly metaphyseal and more likely to occur in the extremities. A family history of other sarcomas, leukemias, breast cancers, or adrenal cancers suggests the possibility of Li-Fraumeni syndrome, a tumor predisposition syndrome which occurs as a result of mutations in the p53 gene. It is associated with an increase in the incidence of osteosarcoma but is not associated with Ewing sarcoma. Other less common features include other pituitary hormonal abnormalities, gingival ulcerations with premature tooth eruption, chronic otitis media, and persistent seborrheic rashes. Letterer-Siwe disease is characterized by more severe visceral involvement, including lung, liver, intestinal, and marrow disease, with persistent fevers, irritability, failure to thrive, malabsorption, pancytopenia, and other symptoms related to diffuse organ involvement. Symptoms include fever, hepatosplenomegaly, skin rashes, and meningeal inflammation with meningismus and, potentially, seizures. Laboratory features include pancytopenia, hypertriglyceridemia, hypofibrinogenemia, hyperferritinemia, and hypoproteinemia. Exposure of the patient to blood products from relatives should be avoided to prevent alloimmunization of the patient to potential bone marrow donor antigens. Furthermore, patients receiving chemotherapy often require frequent blood product transfusions, and so exposure to unrelated donors should be minimized as much as possible. Therefore, platelet apheresis units, which are isolated from single donors, are preferred over units pooled from multiple donors. Platelet transfusions should be given to prevent spontaneous hemorrhages when the platelet count is lower than 10,000/L. In most cases, a lumbar puncture can be performed safely with platelet counts higher than 10,000/L. Intramuscular injections should be avoided when platelet counts are less than 20,000/L. To prevent intracranial hemorrhages in patients with brain tumors, the platelet count should be higher than 30,000-50,000/L. Lower extremity blockade: femoral blood pressure medication protocol order innopran xl 40 mg free shipping, sciatic arrhythmia examples purchase innopran xl without prescription, and lateral femoral cutaneous nerves arrhythmia kamaliya order innopran xl american express. Become skilled in discontinuing anesthesia and monitoring emergence from anaesthesia a arteria palatina ascendens generic 80 mg innopran xl overnight delivery. Reversal of neuromuscular blockade Course and Curriculum of M D Anaesthesiology 11 b. Become skilled in use of techniques for conscious sedation and monitored anaesthesia care a. Know how to successfully resuscitate, and develop skill of Basic Life support and Advance Cardiac Life support. Radiology and interventional neuroradiology: Know special anaesthetic considerations in these settings: a. Transurethral resection of the prostate: recognize and treat hyponatermia; know different anesthetic options and advantages and disadvantages of each b. The resident will be evaluated every 3 months end posting by all attending consultants who worked with them. The attending physicians complete a Departmental Resident Evaluation Form, which is reviewed by the Clinical Competence Committee. Trauma & Resuscitation All residents must achieve basic and advanced cardiac life support, advanced trauma life support, and pediatric life support training. Acquire Improve ability to evaluate & triage the patient and formulate anesthetic plans, especially in the trauma patient. Manage anesthesia for severely traumatized patients by doing the following as rapidly as possible: 1. Goals Understand the importance, purpose, and components of the anesthesia record and the report from the anaesthetizing anesthesiologist. Respiratory Recognition and acute management of Acute and chronic respiratory failure Status asthmaticus Smoke inhalation and airway burns Upper airway obstruction, including foreign bodies and infection Near drowning Adult respiratory distress syndrome. Should be able to prescribe drugs based on Principles of Drug dosing in renal failure Should know when to use Dialysis/hemofiltration. Central Nervous System Recognition and Acute management of Coma, Drug overdose know Glasgow Coma Scale Metabolic and Endocrine,emergencies like Diabetic ketoacidosis Hypoadrenal crisis, pheochromocytoma. Infectious disease Recognition and acute management of hospital acquired and opportunistic infections, including acquired immunodeficiency syndrome. Should know how to protect against cross infection Infection risks to healthcare workers. Hematologic disorders Recognition and acute management of Defects in hemostasis Hemolytic disorders should be able to prescribe component therapy based on the results of Coagulation profile. Thrombotic disorders sould be able to diagnose Deep Vein thrombosis and know Principles of Anticoagulation and fibrinolytic therapy. Know the indications of Plasmapheresis for acute disorders, including neurologic and hematologic. Gastrointestinal disorders Sould be able to recognize and manage Gastrointestinal bleeding hepatic failure should be able to prescribe prophylaxis against stress ulcer bleeding. Factors producing errors in cardiac output measurements Course and Curriculum of M D Anaesthesiology 15 C. Know how to use invasive monitoring devices to guide therapeutic use of fluids and inotropic drugs D. Know how to use arterial blood gas and ventilatory variables to evaluate postoperative patients with respiratory failure 2. Understand the operation of mechanical ventilators including different ventilatory modalities and how each is best used for management of respiratory failure and noninvasive) including modes complications and modes of weaning Principles & application of Oxygen therapy. Recognize sepsis in the postoperative patient including all the typical hemodynamic findings 2. Use various monitoring devices to assist in managing sepsis; specifically understand the optimization of oxygen delivery to tissues in the septic patient and the appropriate management of fluids and vasopressors to accomplish these goals. Know the different classes of antibiotics and antifungal agents and their use in treating sepsis F. Learn about the use of enteral nutrition in the patient who cannot tolerate input per os 2. Learn about the use of parenteral nutrition in the critically ill surgical patient 3. Interact with nutrition support services in planning nutrition for the critically ill patient G. For Patient on Ventilator Principles of Transplantation Care of Immunosuppression Infections in the immunocompromised patient Should know Organ rejection. In addition to practical training in the following procedural skills, the resident must have an understanding of the indications, contraindications, complications & pitfalls of these interventions. Understand cardiac physiology Develop knowledge of cardiovascular anesthesia (anesthesia for the patient with cardiovascular disease). Choose appropriate anesthetic techniques for patients with different types of cardiovascular disease and the skills for lifelong continuing education. Develop technical and monitoring skills necessary for cardiovascular anesthesia C. Administer anesthesia for a wide variety of cardiothoracic Cases and develop interest in further learning D. Perform a thorough preoperative assessment of the patient undergoing cardiovascular surgery E. Know intraoperative anesthetic management for the patient undergoing cardiopulmonary bypass. Know how cardiopulmonary bypass is instituted and discontinued Understand cardiopulmonary bypass and discuss the mechanical aspects of it as follows: 1. Effects of bypass on volumes of distribution and clearance of anesthetic drugs and anesthetic maintenance, including amnesia D. Know how and why to use of inotropic support, vasodilators, and antiarrhythmic drugs that may be Course and Curriculum of M D Anaesthesiology 17 necessary before but are especially necessary after cardiopulmonary bypass E. Develop and understanding of the major issues involved in the perioperative care of the child with congenital heart disease B. Insert vascular catheters or cannulas for adult and pediatric patients and obtain measurements from them as follows: 1. Postcardio;ulmonary bypass coagulopathy Rationale for various therapies such as aprotinin designed to prevent Coagulopathy G. Work as a team member with fellow anesthesiologists, surgeons, perfusionists, and nurses I. Maintain good clinical judgment under stress and act quickly and accurately in diagnosis, interpretation, and treatment of intraoperative problems Evaluation to Determine Goal Achievement. Know the effect(s) of commonly used anesthetic agents and adjuvant agents, for example antihypertensives, on cerebral physiology. Understand the anesthetic implications of the most common neurosurgical procedures, that is, what is likely to happen during neurosurgery that will affect anesthetic management. Understand the basic concepts behind electrophysiologic monitoring of the brain and spinal cord. Understand how concurrent medical illnesses affect anesthesia during neurologic surgery. Review the medical history and physical examination of patients; assess their major neurosurgical problem. Evaluate the patients Glasgow Coma Scale as well as other medical problems that may affect anesthetic care; and know what information about nervous system function and pathology as important to the anesthesiologist. Evaluate the patient with subarachnoid hemorrhage and intracranial aneurysm by means of the Hunt-Hess and Fischer gradings systems; recognize preoperative vasospasm; and anticipate which patients are likely to require special techniques such as barbiturate protection, hypotension, induced hypertension, or temporary vessel occlusion. Differentiate between radiculopathy and myelopathy and understand the anesthetic implications of each, that is, which patients require awake intubation and positioning. Acoustic neuroma, Ependymoma, Gliomas, Meningioma, Pituitary tumours Understand the following different types of spinal operations as well as their anesthetic implications: a. Anterior cervican discectomy and fusions, anterior cervial corpectomies, posterior cervical fusions, laminectomies, and foramenotomy, Laminectomies for excision of spinal cord tumors, both intrameullary and extramedullar, Lumbar laminectomies, microdiscectomies, corpectomies, and fusions with instrumentatio, Thoracic laminectomies and discectomies. Anticipate premedication for and anesthetic considerations during electrocorticography 7. Anticipate airway and sedation requirements for stereotactic neurosurgical procedures conducted with either general anesthesia or monitored anesthesia care Perform the following specific procedures and monitoring techniques necessary to care for the neurosurgical patient. Choose appropriate premedication and agents for anesthetic induction and maintenance based on a knowledge of their effects on cerebral physiology and on neuropathology 2. Discount innopran xl 40mg overnight delivery. SmartHeart Digital Wrist Blood Pressure Monitor.
She has palpable purpuric lesions blood pressure categories buy innopran xl 80mg fast delivery, coalescing by the ankles heart attack young man order innopran xl master card, and ascending up to the buttocks hypertension reading chart proven innopran xl 80 mg. An 18-month-old boy was healthy until the acute onset of persistent fevers 4 days ago pulse pressure 90 innopran xl 80 mg with mastercard. His mother brings him to the emergency department and you note an exanthem on the trunk. You may expect to see all but which of the following findings on your admission physical A 15-year-old girl has had Raynaud symptoms for 1 year, and she occasionally develops sores on her fingertips. Over the past 6 months, she developed fullness of her fingers with skin tightening and decreased finger-joint range of motion. In the past 6-12 months, an 8-year-old boy developed an altered appearance of his lower right leg including tautness and shininess of the skin and decreased ankle range of motion. It is important to have a broad differential when first assessing this type of patient. Children with leukemia may present with musculoskeletal pain that is frequently out of proportion to the physical findings. This diagnosis may be overlooked in those who do not have blasts on peripheral smear (approximately 15% of children). Although some patients may present with nephrotic syndrome, hypertension, and renal insufficiency, the majority initially have no clinical symptoms of renal disease. Therefore, it is important to perform frequent urinalyses, assess protein excretion (the easiest way is by performing a protein-to-creatinine ratio on a spot urine), and follow the serum creatinine and albumin. In addition to histologic classification, activity (inflammation) and chronicity (scarring) indexes are also assessed, which have a further impact on medical treatment decisions and renal prognosis. Lupus nephritis is associated with increased morbidity and decreased long-term survival. The poorer outcome is related to renal complications such as hypertension, nephrotic syndrome, and renal failure. To help protect inflamed and compromised kidneys, blood pressure management is essential. If progression to renal failure occurs, the patient undergoes dialysis until a transplant can be performed. Fortunately, clinically significant lupus nephritis occurs in less than 5% of transplanted kidneys. Both are nonspecific studies affected by infection and other inflammatory conditions. These include growth suppression (starting at doses equivalent to 3 mg/day in small children), musculoskeletal (osteoporosis, avascular necrosis, muscle wasting, myopathy), cardiovascular (hypertension, hyperlipidemia), ophthalmologic (cataracts, glaucoma), skin (striae, impaired healing), diabetes, secondary adrenocortical insufficiency, and immunosuppression. Hydroxychloroquine is often effective in treating skin, muscle, and joint involvement. Ten-year survival has increased from less than 50% in the 1950s to more than 90% currently. Primary Raynaud is most common in adult women, usually during their third and fourth decades of life. It may occur in teenage girls but is rare in prepubertal children and teenage boys. In both primary and secondary Raynaud, the triphasic color change, in order, is white > blue > red. The pathogenesis is arterial vasoconstriction with subsequent reduction in local blood flow, particularly to the hands, the toes, and occasionally the ears, nose tip, and lips. It is important to know if a child with Raynaud has a primary or secondary process. The history, physical examination, and laboratory evaluations are all essential to help determine this. Treatment includes patient education to keep the extremities warm and the core temperature up, vasodilators (such as calcium channel blockers), and biofeedback. Proximal muscle weakness, muscle tenderness, and active skin lesions, including diffuse cutaneous vasculitis and erythema over the extensor aspects of the elbows and knees may be present. The diagnosis requires the presence of the classic rash consisting of Gottron papules that are scaly, erythematous lesions over the dorsal aspects of the metacarpophalangeal and interphalangeal joints (Figure 141-2), and a heliotrope discoloration over the upper eyelids, often with mild periorbital edema. It may be difficult to evaluate the presence of muscle weakness in a child younger than 7 years of age in whom it is often not possible to perform formal muscle strength grading. Therefore, assessment of gross motor skills (such as the ability to squat and arise, balance, jump, hop, get on and off the floor, and ascend stairs) is an essential part of the physical examination. The risk of aspiration is quite real in these patients who require aggressive medical management and may need protection of the airway. Currently, long-term survival is more than 95%, and more than two-thirds of patients have good to excellent outcomes. Calcinosis is still a major cause of morbidity and reflects prolonged periods of poorly controlled disease (Figure 141-3). Radiograph showing extensive calcinosis in the lower leg muscles and fascial planes of an adolescent with long standing, poorly controlled dermatomyositis. Distribution is primarily over the dependent areas of legs (especially prominent by the ankles) and buttocks, but it may also occur on the hands and arms. Recurrence of the purpuric rash, especially after increased physical activity, is common during the first 6 weeks. Subcutaneous edema may be present in younger children and occurs on the dorsum of hands and feet, periorbital areas, scalp, and scrotum. Arthritis, most commonly involving ankles and knees, occurs in 60-80% of children. A reasonable treatment regimen is 1-2 mg/kg per day for 1 week, tapering off over the next few weeks. Mild proteinuria may also be present, but nephrotic syndrome, renal insufficiency, and hypertension are uncommon. Early renal characteristics associated with persistent nephropathy or renal failure include proteinuria more than 1 g/day, nephrotic syndrome, and renal insufficiency. Its pathology includes vasculitis and fibrinoid necrosis of medium-size arteries, especially the coronary arteries. This treatment is especially effective when given within 10 days of presentation, usually resulting in immediate defervescence and a marked decrease in the risk of developing coronary aneurysms (from >20% to <5%). Some patients require further treatment, usually high-dose intravenous methylprednisolone. High-dose aspirin (80-100 mg/kg/day) is also given during the acute phase and then decreased to antiplatelet dosing (3-5 mg/kg) until acute-phase reactants and platelet levels return to normal. Long-term sequelae occur most often in patients who were diagnosed with giant aneurysms (internal vessel diameter 8 mm) during the acute illness. These patients may develop vessel stenosis and occlusion, leading to ischemia and/or infarction. The pathology of systemic and localized scleroderma is similar, with early inflammatory infiltrate in the skin and other involved tissues, followed by increased fibroblast and collagen deposition. Raynaud, present in more than 90%, is often severe, resulting in digital ulcerations and gradual loss of distal tufts (Figure 141-5). Initially, tense swelling with subcutaneous edema, especially of the fingers and arms, is prominent. Then the skin gradually tightens down, resulting in marked limitation in finger and large joint range. Pulmonary disease is present in most patients and can be asymptomatic or characterized by dyspnea on exertion or dry cough. Lung involvement may be primarily parenchymal with fibrosis, vascular leading to pulmonary hypertension, or a combination of both. Serial pulmonary function tests are indicated during the course of the disease to evaluate for restrictive disease and decreased diffusion. Radiographic studies, especially to assess esophageal function, may be helpful in guiding treatment.
In 2011 grad Professional Psychology: Research and Practice arrhythmia university discount 40mg innopran xl fast delivery, 22 blood pressure medication makes me tired order innopran xl cheap, uate study in psychology arrhythmia unspecified icd 9 code purchase on line innopran xl. The internship crisis: A call to Substance Abuse and Mental Health Services action hypertension 14090 order innopran xl 40 mg line. It includes procedures, policies, and regulations for the Department, College, and University of Florida. All students should familiarize themselves with this handbook, as well as with the University of Florida and Graduate School policies. Important links you should familiarize yourself with are: Ethical Principles of Psychologists and Code of Conduct. On a daily basis, we focus upon the integration of science and practice in all our activities. The faculty, staff, graduate students, interns, post doctoral fellows and alumni of the Department seek to maintain and advance our state-wide, national and international reputation as a "Center of Excellence" in psychological science, education and service delivery. College of Public Health and Health Professions Mission the mission of the College of Public Health and Health Professions is to preserve, promote and improve the health and well-being of populations, communities and individuals. To fulfill this mission, we foster collaborations among public health and the health professions in education, research and service. Goals Goal I: Provide excellent educational programs that prepare graduates to address the multifaceted health needs of populations, communities and individuals. Maintain and enhance excellent academic programs that emphasize current knowledge, discovery and practice 4. Develop and maintain partnerships with community organizations to promote health 2. These features foster program strengths in research, teaching, and professional training in health care psychology. The graduate of this training model is capable of functioning as an investigator and as a practitioner, and may function as either or both, consistent with the highest standards in psychology. The scientist-practitioner model is ideal for psychologists who utilize scientific methods in the conduct of professional practice. To accommodate the broad range of career trajectories possible within scientist-practitioner education and training, the program offers a flexible Scientist-Practitioner curriculum that allows students to obtain broad research, clinical, and academic training that readies them for careers anywhere along the science-practice continuum. Beyond the core require rments of the program, students are allowed some degree of flexibility in developing an individualized plan of study that prepares them for their intended career path. Some students may elect to focus more intently on developing broad evidence-based assessment, intervention, or consultation skills in health service psychology, while others may elect to focus more intensively on the acquisition of research skills, training in scientific methods and technologies in preparation for an academic research career. Curricular planning together with the mentor and supervisory committee allows the student to obtain broad professional training that features increasing levels of independent functioning in health service psychology, or to obtain more intensive research and technical skill while spending less time in clinical training with the general faculty. Regardless of which path the student chooses, developing academic competencies in core areas of psychological and clinical psychological science and practice, competencies in research and knowledge dissemination, and competencies in health service delivery are built in all graduates. It is expected that all graduates of the doctoral program will have the necessary background to seek licensure and board certification in relevant areas. All students admitted to graduate study in the Department of Clinical and Health Psychology are expected to work toward the Ph. The program is designed so that the student can master broad areas of knowledge in psychology and clinical psychology, can demonstrate competency to contribute to the knowledge base of the field through research and scholarship, can develop professional knowledge, skills and attitudes in psychological assessment, consultation and intervention, and can develop an appreciation for the role of cultural diversity in research and clinical work while obtaining 1 knowledge and practical skills in a defined major area of study. The doctoral program is comprised of core requirements along with elective study areas chosen by the student. The following regulations apply specifically to the 2019-2020 entering class in the Department of Clinical and Health Psychology and are in addition to those in the Graduate School Catalog and those summarized in the Graduate Student Handbook. Requirements for previous cohorts are outlined in the handbook they received at the time of their first registration. All students should retain a copy of the student handbook that applies to their entering class. Please be sure to keep these documents on hand, and review them on a periodic basis. Updates and additions will be provided throughout the course of graduate study, and it is up to the student to keep their handbook current by adding new policies to it. With regard to program requirements, students are responsible for fulfilling those requirements in place at the time of matriculation. The Clinical and Health Psychology graduate student is also responsible for knowledge of the ethical principles and standards of the American Psychological Association and is bound to these as guidelines in their role as a student. Graduation from the doctoral program in clinical psychology does not by itself qualify a person to practice as a psychologist, nor does it guarantee that the graduate will pass all requirements or be eligible for licensure in all states. The Graduate School is responsible for the enforcement of minimum general standards of graduate work throughout the University. The responsibility for the detailed operations of graduate programs is vested in individual Colleges and Departments. The Department of Clinical and Health Psychology administers the Doctoral Program in Clinical Psychology. The program has been continuously accredited by the American Psychological Association since 1953. We were recently reaccredited and will retain accreditation status until our next self-study/site visit in 2022. The Department is housed in the College of Public Health and Health Professions in the University of Florida Academic Health Center. The Department operates the Psychology Clinic, the primary resource for academic and clinical expertise regarding biopsychosocial aspects of health and illness at the Academic Health Center. In addition to the clinic, students often obtain supervised clinical experience in outpatient or community-based clinics, inpatient units, and other off-campus facilities including the Malcom Randall Department of Veterans Affairs Medical Center. More than 200 applications for admission are received each year from students in universities throughout North America and other countries. Currently there are 72 students in the doctoral program, including those who are off-campus completing their internships and dissertation research. Lori Waxenberg, that attract students from doctoral programs throughout the country. The integrated training experiences of the department place post-doctoral fellows, interns and graduate students together on vertical teams, to the benefit of all. The health care setting, the independent departmental status of Clinical and Health Psychology, and the integration with a nationally recognized pre-doctoral internship program all enhance our educational mission and are all unique features in current graduate education in psychology. Faculty the term "core faculty" is used to describe faculty who have major education and training functions within the two departmental programs. Some of these faculty members are on the Tenure Track, while others are on the Single Mission or Multi-Mission Track. Core faculty members play integral and varied roles in the education and training of graduate students. Nearly all core faculty are licensed psychologists who are involved in clinical practice, supervision, teaching and scholarly activities. A number of additional faculty in other units of the Academic Health Center or University play roles in the didactic, clinical and research training program. See Appendix A for a listing of graduate faculty and a sample of their current activities. A vita for each faculty member is available for your review on the department website at chp. With staff assistance, students are expected to play an active role in assuring accurate and up-to-date record-keeping to enable continuous quality improvement efforts. Periodic reminders will be given to students to review their file prior to annual reviews, internship applications, or other major milestones. A current list of contact information for faculty, interns, students, and staff can be found on the intranet portion of our website internal. Because this information is continuously updated, students should utilize the link on the department intranet to ensure they have the most updated information. In order to access the department intranet you must have a Gatorlink account set up. The Department will submit authorization and payment for your Gator1 card to the bookstore, however if your card is lost or stolen, the student will be responsible for replacement fees. |